As cannabis rounds the bend in many states toward legalization, one of the biggest questions on society’s mind is how to ensure that it is safe and does not impair potential life threatening activities. Since the founding of MADD in 1980, we’ve grown more aware of the danger of drunk driving, which kills close to 28 people a day in America and is a heart-breaking drain on society. Since cannabis can also have mind-altering effects, as a society, we’re equally wary about the danger of driving under the influence of cannabis or any psychoactive substance for that matter. In fact, this fear is constantly cited as reason for not passing medical cannabis legislation. This concern has led states that have already approved medical cannabis to pass regulations specifying levels acceptable for operating vehicles.
At first glance, this all seems acceptable. In the same way that patients with allergies should not take Benadryl before operating machinery, medical cannabis patients must be careful about actions that can jeopardize their safety or the safety of others. However, some of these legal driving limits are unbelievably low. In Washington State, for example, the legal limit is 5 nanograms THC-COOH per milliliter of blood in a blood test. To put that in perspective, this amount could actually exist in a medical cannabis patient 24 hours after consuming cannabis. But is a patient realistically an inhibited driver 24 hours after medication? Of course not. Anyone with a proper medical cannabis experience knows that. However, that’s just the question. How does cannabis actually affect driving in regular medical cannabis users? What is safe? How do we make these types of regulations as a society?
The problem is somewhat difficult to answer; studying car drivers in real life is obviously unethical, due to the risk of accident. To get around this issue, one medical group at the University Hospital of Dusseldorf (Germany) set out to study the question by assessing bicycle riders performance before and after consumption of cannabis. Fourteen regular cannabis users (12 male and 2 female) with an average age of ~25 years old participated in this study. “Regular user” was defined as anywhere from 1 gram a week (light use) to 1 gram a day (heavier use). The users were then subjected to a battery of evaluations on a closed, dry, test course. The test course included simple tasks, such as weaving around regularly and irregularly spaced obstacles, riding for 45 meters on a narrow track, and circling clockwise, but also included more complex tasks that more accurately mimic real-world driving conditions, such as traffic lights, memory of a random word displayed on an LED, a ball suddenly rolling in front of the bicycle, the glare of a torch light, and auditory disturbances!
Below is a map of the course used:
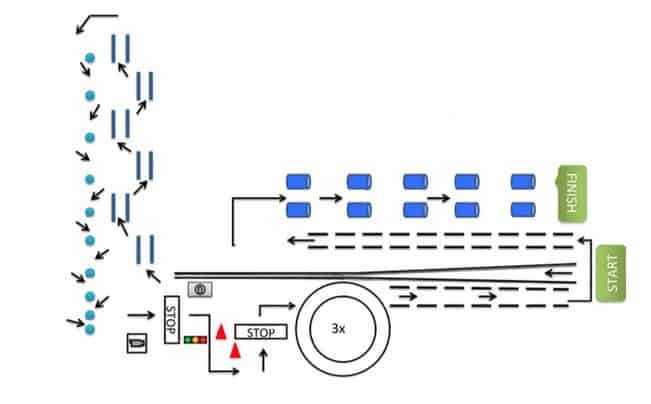
Dutch medical cannabis from Bedrocan was used at a consistent quality. Test subjects were allowed to warm up briefly then were recorded riding the track for an initial evaluation of sober ability. After this, each subject consumed a cannabis cigarette and repeated the course immediately. Subjects could then stop the test or smoke yet another cigarette and repeat the course. In this manner, participants could choose to smoke and repeat the trial a total of three times in a row. Two hours after the last consumption, participants were then tested on the course for a final time to establish the latent effects of cannabis on cycling ability. This setup ensured that all participants had data of test runs both without and with cannabis consumption immediately prior. The setup also allowed heavier users to consume up to an amount that would represent peak psychoactivity. In other words, both light and heavy consumption could be studied. After each ride, a medical report for the suspicion of driving under the influence of drugs or alcohol was performed and a blood sample was taken, much in the same way police might subject erratic drivers to similar testing.
Researchers made evaluation of the test course performance as objective as possible. Faults were separated into three categories:
1) Coordinative faults – leaving the track with both wheels or one wheel, pushing over a barrel, skipping an obstacle, driving in meandering lines
2) Concentrative faults – running a red light, running a yellow light, inadequate waiting at a green light, missing the correct number of circle rounds, and missing the word on the LED display
3) Complex situation faults – failure to stop before the rolling ball, etc.
Performance during consumption was then expressed as a percentage of the score observed during the sober test to help show the relative change in driving ability. As it turned out, “hardly any coordinative disturbances could be detected under the influence of high or very high THC [blood] concentrations.”
The graph below in fact shows driving performance as a percentage of sober performance for three levels of THC:

As you can see, the negligible difference is actually positive for higher levels! Since cannabis has been shown to affect basic motor coordination in other circumstances, this data might therefore suggest that cannabis patients are compensating for the effects of cannabis with increased concentration. Cycling speed was not included as an aspect of this study, so additionally, it’s possible that cyclists under the influence were also riding more slowly. However, the basic message is clear: cannabis consumption does not seem to cause an issue in driving-related coordination, even at high levels. A genuine association has yet to be proven.
Of course, patients and states should interpret this data very cautiously. For one, a potential flaw in the design is that test subjects became increasingly knowledgeable to the course with each run. Readers might imagine that the first run of a course would not go as smoothly as repeat attempts, meaning that difference between sober and non-sober driving might be minimized in this study. Additionally, as we commonly point out about medical studies, <20 subjects is a small number of test subjects. Finally, the speed of cycling is usually nowhere near the speed of automobile driving. So to be perfectly clear about our position: patients should always, always exercise extreme caution when driving. The cost/benefit of getting somewhere 10 minutes early is not worth the risk of ending your own life or the lives of other drivers.
Regardless, it seems like medical cannabis states might need to re-evaluate driving regulations to prevent medical patients from unfairly being subject to penalties for driving under the influence while their abilities are not actually affected.
Works Cited
Benno Hartung, Holger Schwender, Eckhard H. Roth, et al. (2015) The effect of cannabis on regular cannabis consumers’ ability to ride a bicycle. International Journal of Legal Medicine (2015). DOI: 10.1007/s00414-01501307-y.